Mayo Clinic researchers reported a strong hint that blood plasma from COVID-19 survivors helps other patients recover, but it’s not proof and some experts worry if, amid clamor for the treatment, they'll ever get a clear answer.
More than 64,000 patients in the U.S. have been given convalescent plasma, a century-old approach to fend off flu and measles before vaccines. It's a go-to tactic when new diseases come along, and history suggests it works against some, but not all, infections.
There’s no solid evidence yet that it fights the coronavirus and, if so, how best to use it. But preliminary data from 35,000 coronavirus patients treated with plasma offers what Mayo lead researcher Dr. Michael Joyner on Friday called “signals of efficacy.”
There were fewer deaths among people given plasma within three days of diagnosis, and also among those given plasma containing the highest levels of virus-fighting antibodies, Joyner and colleagues reported.
The problem: This wasn’t a formal study. The patients were treated in different ways in hospitals around the country as part of a Food and Drug Administration program designed to speed access to the experimental therapy. That so-called “expanded access” program tracks what happens to the recipients, but it cannot prove the plasma — and not other care they received — was the real reason for improvement.
Rigorous studies underway around the country are designed to get that proof, by comparing similar patients randomly assigned to get plasma or a dummy infusion in addition to regular care. But those studies have been difficult to finish as the virus waxes and wanes in different cities. Also, some patients have requested plasma rather than agreeing to a study that might give them a placebo instead.
“For 102 years we’ve been debating whether or not convalescent plasma works,” said Dr. Mila Ortigoza of New York University, referring to plasma’s use in the 1918 flu pandemic. This time around, “we really need undisputable evidence.”
Ortigoza is co-leading one such study, which this week is expanding to three other states — Connecticut, Florida and Texas. Her team also is working to pool data with several other clinical trials in other regions, in hopes of faster answers.
“There’s concern about when there will be a clear answer,” agreed infectious disease specialist Dr. Jeffrey Henderson of Washington University in St. Louis.
He’s hopeful the clinical trials will push forward but said the Mayo report is consistent with smaller, earlier plasma studies and "an example of making the best you can of the data that’s available."
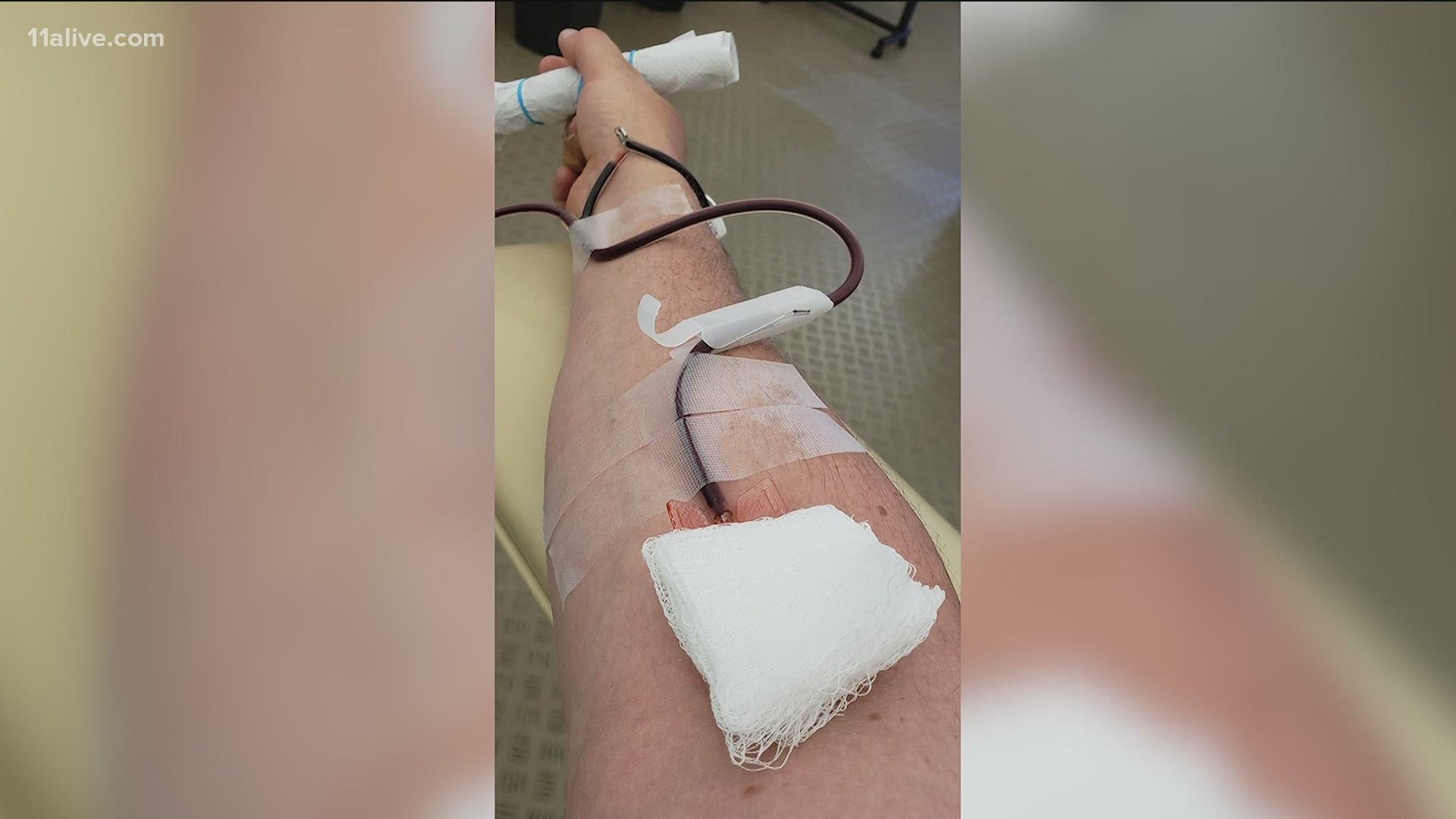
When the body encounters a new germ, it makes proteins called antibodies that are specially targeted to fight that particular infection. The antibodies float in plasma — the yellowish, liquid part of blood. Because it takes a few weeks for antibodies to form, the hope is that transfusing someone else’s antibodies could help patients fight the virus before their own immune system kicks in.
The Mayo findings were posted online ahead of scientific peer review. They show that 20% of people given high-antibody plasma within three days of diagnosis had died within 30 days compared with 30% of people treated later with low-antibody plasma.
The FDA has been closely considering if the evidence is good enough to allow so-called emergency use of convalescent plasma, a step that would make it even harder for more rigorous testing to be completed. FDA didn’t immediately comment Friday.
Tens of thousands of COVID-19 survivors have donated their plasma, and blood banks have issued calls for even more to meet the demand as the coronavirus continues to ravage the U.S. According to AABB, the American Association of Blood Banks, a quarter of hospitals it checks weekly are reporting waits of more than 24 hours in obtaining requested plasma.
Beyond whether plasma generally helps, scientists want to know when it should be used — for the very sick or at the earliest sign of infection? And what’s the right dose? COVID-19 survivors harbor widely varying amounts of antibodies, which Ortigoza said is difficult to measure before the donated plasma is used. She said another question is which of the many types of antibodies are the best to use.
Joyner noted that the expanded access program wasn’t meant to replace rigorous studies but was originally designed to track 5,000 people and see if plasma was safe. Instead, the program skyrocketed.
“There’s probably reasonable, actionable evidence from our findings to really reaffirm” historic lessons of plasma therapy, that earlier use is better, he said.

